

Meta description: Understand the main types of obesity and how effective treatment is chosen according to guidelines used in the United States, Canada, and Asian populations.
Introduction
Obesity is not simply a matter of body weight. It is a chronic, complex, and multifactorial disease involving excess or dysfunctional adipose tissue, metabolic changes, inflammation, appetite regulation, genetics, sleep, stress, environment, and lifestyle.
Current international guidelines increasingly recommend treating obesity according to health risk, fat distribution, complications, and individual patient profile, not only by body mass index (BMI). In the United States and Canada, obesity is generally defined as BMI ≥30 kg/m², while many Asian populations use lower BMI thresholds because cardiometabolic risk may appear at lower body weights.
This article explains the main types of obesity and how treatment can be matched to each clinical situation, including lifestyle therapy, anti-obesity medications such as GLP-1 receptor agonists, and bariatric/metabolic surgery.
What Are GLP-1 Medications?
GLP-1 medications are drugs that mimic or enhance the action of incretin hormones involved in appetite, satiety, gastric emptying, and glucose regulation.
The best-known examples include:
- Semaglutide — Wegovy/Ozempic
- Liraglutide — Saxenda/Victoza
- Tirzepatide — Zepbound/Mounjaro, dual GIP/GLP-1 action
In obesity treatment, GLP-1-based therapies are not “cosmetic weight-loss injections.” They are medical treatments used for selected patients with obesity or overweight plus health complications, always combined with nutrition, physical activity, behavioral changes, and clinical monitoring. The Endocrine Society recommends that diet, exercise, and behavioral strategies remain part of all obesity treatment approaches.
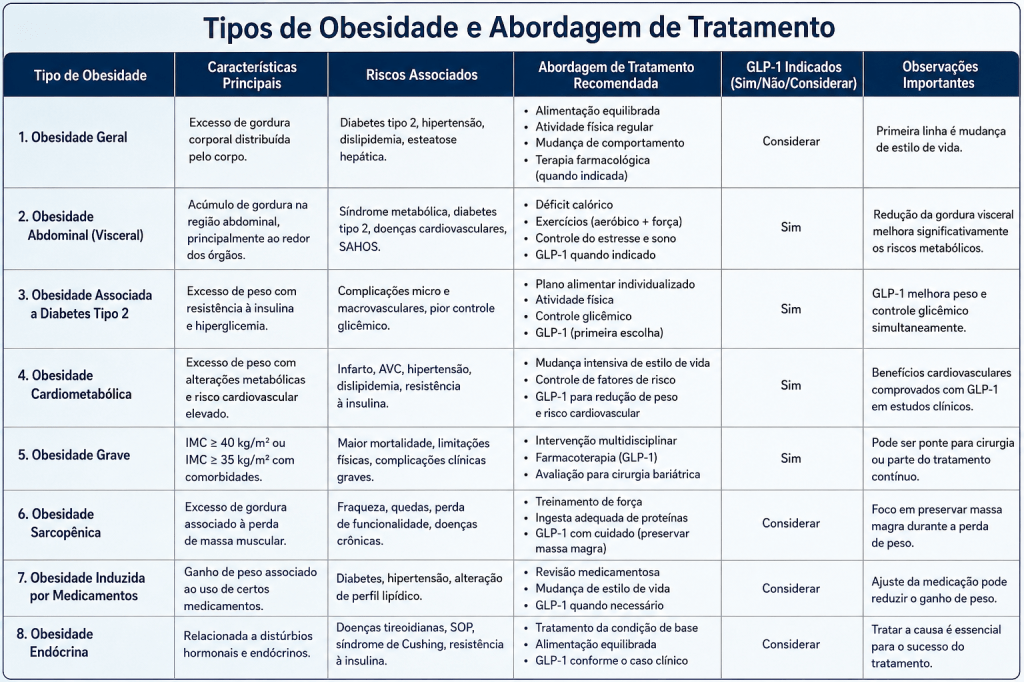
Main Types of Obesity and Effective Treatment
1. General Obesity
General obesity refers to increased total body fat, commonly identified by BMI.
In many Western guidelines:
- Overweight: BMI 25–29.9 kg/m²
- Obesity: BMI ≥30 kg/m²
In Asian populations, risk may occur at lower BMI levels, and many countries use BMI thresholds such as 25 or 27.5 kg/m² for obesity risk classification.
Most effective treatment
The foundation is:
✅ calorie-controlled, nutrient-dense diet
✅ resistance training and aerobic activity
✅ sleep improvement
✅ behavioral therapy
✅ treatment of associated conditions
Medication may be considered when lifestyle therapy alone is insufficient and the patient meets clinical criteria.
2. Abdominal or Visceral Obesity
This is one of the most dangerous forms of obesity. It occurs when fat accumulates around the abdomen and internal organs.
It is strongly associated with:
- insulin resistance
- type 2 diabetes
- fatty liver disease
- hypertension
- cardiovascular risk
- chronic inflammation
For Asian adults, central obesity is often defined using lower waist circumference thresholds, commonly around ≥90 cm for men and ≥80–85 cm for women, depending on the guideline and population.
Most effective treatment
The treatment focus should be cardiometabolic risk reduction:
✅ weight loss of 5–15%
✅ Mediterranean-style or high-fiber diet
✅ reduced refined carbohydrates and ultra-processed foods
✅ strength training
✅ treatment of insulin resistance
✅ GLP-1 or GIP/GLP-1 medications when clinically indicated
This type of obesity often responds well to structured lifestyle therapy plus pharmacotherapy when there are metabolic complications.
3. Obesity With Type 2 Diabetes
This is a high-priority clinical category because excess adiposity and insulin resistance reinforce each other.
In patients with diabetes and obesity, GLP-1 receptor agonists and related therapies are frequently prioritized because they can support:
- weight reduction
- better glycemic control
- appetite regulation
- cardiometabolic improvement
The ADA and other guideline-based reviews recognize GLP-1-based therapies as preferred options for many people with type 2 diabetes and obesity.
Most effective treatment
✅ individualized nutrition plan
✅ glucose monitoring
✅ resistance exercise
✅ metformin when appropriate
✅ GLP-1/GIP-based medication when indicated
✅ blood pressure and lipid control
✅ long-term follow-up
4. Obesity With Cardiovascular Risk
This includes obesity associated with:
- hypertension
- dyslipidemia
- coronary artery disease
- previous cardiovascular events
- sleep apnea
- chronic inflammation
Health Canada approved semaglutide/Wegovy not only for obesity treatment but also for reducing risk of nonfatal heart attack in adults with established cardiovascular disease, reflecting the broader cardiometabolic role of modern obesity treatment.
Most effective treatment
✅ heart-healthy diet
✅ sodium reduction when needed
✅ supervised physical activity
✅ lipid and blood pressure control
✅ GLP-1-based therapy when appropriate
✅ smoking cessation
✅ sleep apnea evaluation
5. Severe Obesity
Severe obesity is usually defined as:
- BMI ≥40 kg/m²
or - BMI ≥35 kg/m² with obesity-related complications
This form often requires more intensive treatment.
Most effective treatment
✅ multidisciplinary care
✅ anti-obesity medication
✅ bariatric/metabolic surgery evaluation
✅ psychological support
✅ nutrition follow-up
✅ long-term vitamin/mineral monitoring after surgery
For many patients with severe obesity, lifestyle changes alone may not be enough. Bariatric surgery remains one of the most effective long-term treatments, especially when obesity is associated with diabetes, sleep apnea, fatty liver disease, or severe mobility limitation.
6. Sarcopenic Obesity
Sarcopenic obesity occurs when a person has excess body fat but reduced muscle mass. It is more common in older adults and people with sedentary lifestyles.
This type is dangerous because the scale may not show the full problem. The patient may lose weight but also lose muscle if treatment is poorly planned.
Most effective treatment
✅ high-protein diet when appropriate
✅ resistance training
✅ vitamin D assessment
✅ fall prevention
✅ avoid overly aggressive calorie restriction
✅ monitor muscle mass, strength, and function
For this group, the goal is not just “weight loss.” The goal is fat loss with muscle preservation.
7. Medication-Induced Obesity
Some medications may contribute to weight gain, including certain:
- antidepressants
- antipsychotics
- corticosteroids
- insulin regimens
- beta-blockers
- anticonvulsants
Most effective treatment
✅ medication review with a healthcare professional
✅ switch to weight-neutral alternatives when possible
✅ lifestyle therapy
✅ obesity pharmacotherapy if criteria are met
✅ avoid stopping medicines without medical guidance
This is a very important point: the patient should never discontinue prescribed medication alone.
8. Hormonal or Endocrine-Related Obesity
Some endocrine disorders can contribute to weight gain, such as:
- hypothyroidism
- Cushing’s syndrome
- polycystic ovary syndrome
- insulin resistance
- menopause-related metabolic changes
Most effective treatment
✅ diagnose and treat the underlying condition
✅ check thyroid function when clinically indicated
✅ manage insulin resistance
✅ individualized nutrition
✅ physical activity
✅ anti-obesity medication when appropriate
In this type, treating only appetite or calories may be insufficient if the underlying endocrine disorder remains uncontrolled.
Treatment Strategy by Clinical Profile
Where GLP-1 Medications Fit Best
GLP-1 medications are generally considered for adults with:
- BMI ≥30 kg/m², or
- BMI ≥27 kg/m² with obesity-related conditions (such as diabetes, hypertension, or dyslipidemia),
alongside comprehensive lifestyle interventions and under medical supervision.
They are not intended as cosmetic weight-loss drugs or stand-alone treatments.
Practical Clinical Approach
Effective obesity management usually combines:
✔ Individualized nutrition
✔ Regular physical activity
✔ Sleep optimization
✔ Stress management
✔ Behavioral counseling
✔ Long-term follow-up
✔ Pharmacotherapy when clinically indicated
Final Conclusion
Obesity is a chronic disease requiring individualized, evidence-based care. Advances in pharmacotherapy—particularly GLP-1 receptor agonists—have transformed treatment options for many patients by improving weight loss and metabolic health when used appropriately.
However, medication alone is rarely sufficient. Sustainable success depends on mi pharmacologic therapy with nutrition, exercise, behavioral support, and long-term medical follow-up.
Understanding the different phenotypes of obesity enables healthcare professionals to select the most appropriate treatment strategy for each individual, maximizing clinical outcomes while minimizing risks.
Scientific References
- American Diabetes Association. Standards of Care in Diabetes.
- American Association of Clinical Endocrinology. Clinical Practice Guidelines for Obesity.
- The Obesity Society.
- European Association for the Study of Obesity.
- World Health Organization.
- National Institute for Health and Care Excellence.
About the Author
Matheus Lucas Araújo Sousa is a licensed pharmacist from Brazil dedicated to translating scientific evidence into clear, practical, and reliable health information. His work focuses on evidence-based supplementation, obesity management, metabolic health, clinical pharmacy, and disease prevention.
Through Strategic Health, his mission is to help readers make informed healthcare decisions using up-to-date scientific research, international clinical guidelines, and practical recommendations that support long-term health and well-being.
Professional Areas of Interest
- 💊 Clinical Pharmacy
- ⚖️ Obesity & Weight Management
- 🧬 Evidence-Based Supplementation
- ❤️ Cardiometabolic Health
- 🧠 Preventive Healthcare
- 📚 Health Education
Disclaimer
This article is intended for educational purposes only and should not replace individualized medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before starting or changing any medication, supplement, or treatment plan.
Strategic Health
Evidence-Based Health Information for Better Decisions.
